



Intraspinal Direct Injection Therapy
傷ついた神経のすぐそばに、幹細胞を直接届けて修復を促す治療法です。
Medical institutions notified by the Ministry of Health, Labor and Welfare※2019年6月〜2026年6月末 東京・大阪・札幌 3院累計
首〜腕・腰〜足 の「しびれ」本当の原因は 『神経へのダメージ』かもしれません
手術をせずに、根本からの回復を目指す。
再生医療(幹細胞治療)という新たな選択肢があります。
87.8%が改善を実感※
※脊髄・脊椎疾患の患者様 追跡調査結果
(大阪院 2020〜2024年)
実際に治療を受けた
患者さまの声
頚椎椎間板ヘルニアの手術後、
手足のしびれが残っていた方が再生医療で改善
腰椎椎間板ヘルニアで下を向いて歩いていた方が、
前を向いて歩けるように
頸椎・腰椎ヘルニア・狭窄症の
症例紹介
実際に当院で再生医療を受けられた患者様の症例をご紹介します

- 頚椎・腰椎ヘルニア・狭窄症・脊髄損傷・脊髄梗塞・脊髄炎などの症例
- Cases of Brain and Spinal Cord Disorders
- Stem cell therapy cases
手術を勧められた頸髄損傷の40代男性が選んだ幹細胞治療という選択肢
手術を勧められた頸髄損傷の40代男性が選んだ幹細胞治療という選択肢 「2ヶ月経っても右手のしびれが取れない。手術しかないのか」――仕事中の転落事故で頸髄損…
2026.08.10
- 頚椎・腰椎ヘルニア・狭窄症・脊髄損傷・脊髄梗塞・脊髄炎などの症例
- Cases of Brain and Spinal Cord Disorders
- Stem cell therapy cases
“リペア幹細胞” 膝下全体のしびれが指先のみに!手術なしで改善!腰部脊柱管狭窄症 80代 男性
膝下全体のしびれが指先のみになった80代男性の腰部脊柱管狭窄症再生治療 「入院や全身麻酔が必要な手術には、なかなか踏み切れない」——。数年前から腰痛と下肢のし…
2026.08.02
- 頚椎・腰椎ヘルニア・狭窄症・脊髄損傷・脊髄梗塞・脊髄炎などの症例
- Cases of Brain and Spinal Cord Disorders
- Stem cell therapy cases
“リペア幹細胞” しびれが軽減し踏ん張りがきくように!排尿も9割回復!頚椎症性脊髄症術後 60代 男性
しびれが軽くなり踏ん張りがきくようになった60代男性の頚椎症性脊髄症術後再生治療 「歩きにくさや手のしびれが、少しでもよくなれば」——。7年前に頚椎症性脊髄症…
2026.07.29
- 頚椎・腰椎ヘルニア・狭窄症・脊髄損傷・脊髄梗塞・脊髄炎などの症例
- Cases of Brain and Spinal Cord Disorders
- Stem cell therapy cases
“リペア幹細胞” 辛い手足のしびれが完全に消失!お出かけを再び楽しめるように!頚髄損傷 70代 男性
手足のしびれ消失で外出を再び楽しめるようになった70代男性の頚髄損傷再生治療 「もうこれ以上の回復は望めないのでは」——。半年前の転落事故で頚髄損傷を受傷した…
2026.07.27なぜリペア幹細胞が
選ばれるのか
当院の幹細胞は、あなたご自身の脂肪から採取し、
生きたまま届ける完全オーダーメイド。
15,000例の治療実績に裏付けられた品質で、
神経の修復に高い効果が期待できます。
1. 冷凍しないフレッシュ細胞
新鮮な、生きた細胞をそのまま投与するので生存率が高い
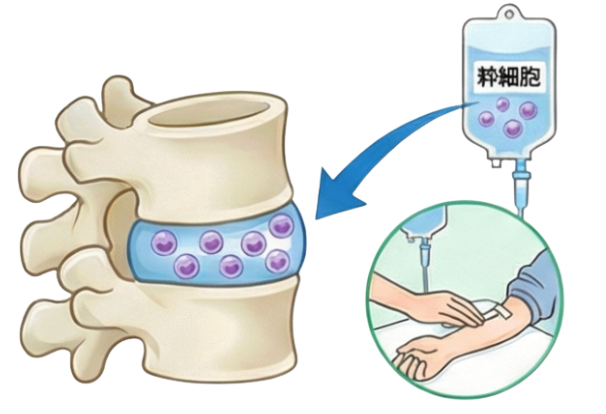
2. 脊髄腔内ダイレクト注射療法
数多くの幹細胞で直接傷ついた神経を再生
3. 1回あたり2億個投与
1億個×2回より高い効果が期待
4. 自己脂肪由来幹細胞
骨髄由来と比較して約2倍の神経修復効果(研究報告)

5. 自己血で培養
牛血清不使用でアレルギーリスクを最小化

6. 化学薬品を使わない培養
独自のシートでダメージを抑え生き生きした細胞をつくる

※各特長の詳細は、下記にてご説明しております。
あなたに当てはまるケースは?
2つのケースから、あなたの状況に近いものをお選びください
手術する前に、知っておいてほしいこと
痛みや痺れに悩んでいる方、手術を勧められているが不安な方へ


こんな状況ではありませんか?
- ✓手術するほどではないが、
痛みや痺れが気になる - ✓手術適応と言われているが、
怖くて手術をしていない - ✓画像ではヘルニアや狭窄はあるが、
症状は落ち着いている
多くの方が実はヘルニアを持っている(無症状)
50代以上の60%以上に椎間板の変化が見つかりますが、その多くは痛みの原因ではありません。肌のシワや白髪が増えるのと同じように、ごく自然な「加齢現象」の一つである可能性が高く、画像で異常が見つかった=手術が必要、とは限らないのです。
※出典:Brinjikji, W., Luetmer, P. H., Comstock, B., et al. (2015). Systematic literature review of imaging features of spinal degeneration in asymptomatic populations. AJNR. American Journal of Neuroradiology, 36(4), 811–816. https://doi.org/10.3174/ajnr.A4173

「症状は軽いのに手術が必要なの?」「手術は怖い…」そんな不安を抱えていませんか。
実は、MRI画像の所見と症状の重さは必ずしも一致しません。
手術の前に、まず知っておいてほしいことがあります。
「手術をしたのに、なぜまだ痛いのだろう...」
手術後も続く痛みやしびれに、不安を感じていませんか


こんな状況ではありませんか?
- ✓術後も痛み・痺れ・筋力低下が続いている
- ✓手術前はなかった症状が出た
- ✓医師から「リハビリか薬で様子を
見るしかない」と言われた
「手術したのに、なぜ…」その落胆と不安、よく分かります。
術後も症状が残る方には、見落とされがちな"もうひとつの原因"があります。
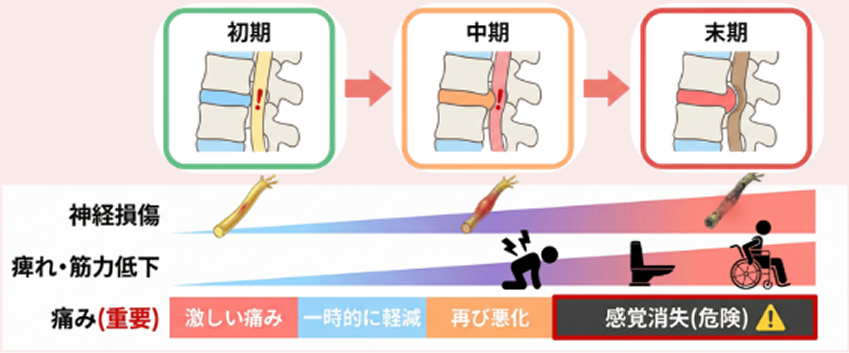
ヘルニアを放置するリスク
「痛み止めで様子をみましょう」そんな経験はありませんか?
実は、痛みが和らいでも体の中ではダメージが進行していることがあります。
放置していると、こんな症状が現れることがあります

靴下を2枚履いている感覚
感覚が鈍くなり、地面に足が着いている
実感がなくなる
排尿・排便のコントロール困難
症状が進行すると、膀胱や腸の機能に
影響が出ることがある
痛みで眠れない・仕事に支障
夜間のしびれで睡眠の質が低下し、
悪循環に陥る
痛みが軽くなった = 治った、ではありません
【例え】虫歯も放置すると...
初期虫歯

痛い
虫歯拡大、
神経が鈍感に
痛みが和らぐ
虫歯が重度、
神経壊死

痛くない
(病気は進行中)
虫歯も最初は痛いですが、
放置すると痛みが消えることがあります。
これは治ったのではなく、
神経が死んでしまったからです。
ヘルニアも同じです。
痛みが和らいでも、
それは「体が治った」のではなく
「感覚が麻痺しているだけ」の可能性があります。
痛みが消えた=安心、ではありません。
本当の原因を知ることが重要です。
放置すると、神経損傷は
初期 → 中期 → 末期
へと進行します
放置すると同じリスクがあります
手術を受けた方も、受けていない方も、放置すれば同じリスクがあります。
早期の診察が、症状悪化の予防につながります。


本当の原因は
神経の損傷
なぜ、手術をしても痛みが残る人がいるのか?
なぜ、注射や薬で一時的にしか楽にならないのか?
答えは、痛みの"本当の発生源"にあります。
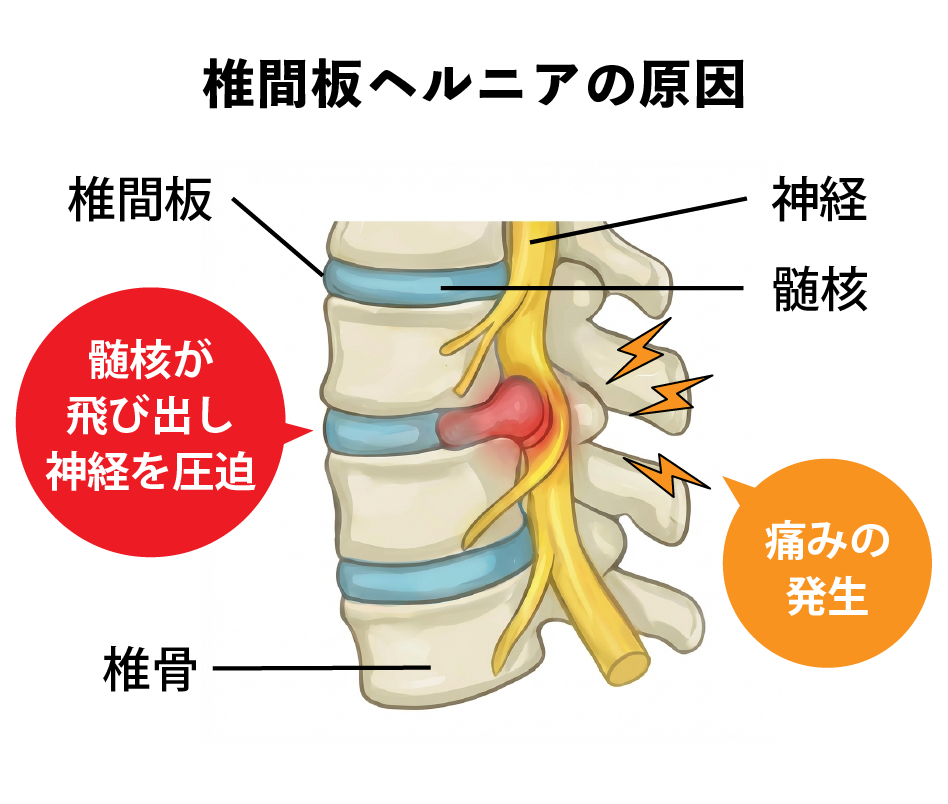
背骨の間にあるクッション(椎間板)の中身、ゼリー状の「髄核」が飛び出して、神経を圧迫している。これがヘルニアと呼ばれる状態です。
確かに、この圧迫は痛みの原因の一つです。しかし、圧迫を取り除く手術をしても痛みが残る人がいます。
それは、圧迫によって神経そのものが傷ついているから。
この「神経の傷」こそが、痛みやしびれの本当の発生源です。
手術で圧迫を取り除いても、
神経の「傷」が修復されなければ症状は改善しません。
幹細胞治療は、この「神経の傷」を修復するアプローチです。
再生医療と手術の違い
神経の傷を修復するには、どんな方法があるのか?
ここでは「再生医療」と「手術」、2つのアプローチの違いを見ていきましょう。
幹細胞投与
〜神経再生・損傷修復〜
傷ついた神経の再生を促し、損傷を修復(脊髄腔内注射)
幹細胞を神経の近くに直接届け、自然治癒力を高めます
椎間板の悪化などを予防(点滴治療)
全身に届く点滴で、広範囲の修復と予防を同時に
procedure
〜圧迫除去には有効・ただし神経修復は困難〜
ヘルニア除去は可能
ただし、傷ついた神経の修復は手術では難しい
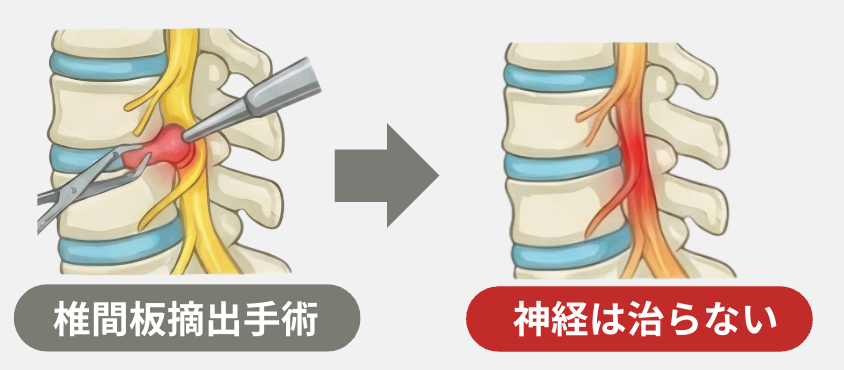
症状残存・悪化・再発のリスクあり
椎間板摘出手術の器具操作
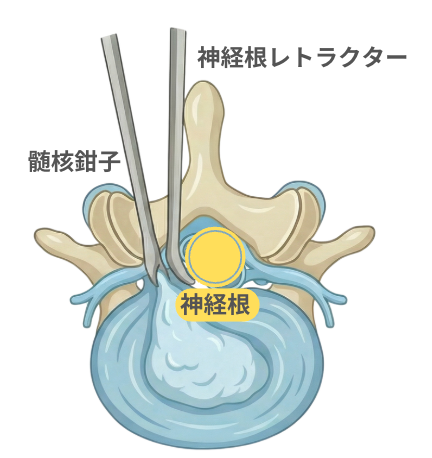
ヘルニアをとるときに器具で神経を避ける際、神経を傷つける可能性
→ 後遺症の原因になることも
手術前で痛みやしびれが気になる方にも効果が期待できる治療法なんだよ!
どのクリニックで受けるかによって大きく変わるんだ。
当院ならではのこだわりを、次で詳しく紹介するね!
まずは無料相談
再生医療が自分に合うか、
専門医に聞いてみませんか?
まずは無料相談で、あなたの症状やお悩みをお聞かせください
無料電話相談 9:00〜18:00
リペアセルクリニックの
6つの特長
再生医療は、どこで受けるかによって結果が大きく変わります。
幹細胞の培養方法は医療機関によって千差万別だからです。
当院独自の「リペア幹細胞」は、あなた自身の脂肪から採取し、
完全オーダーメイド・無添加培養で生きたまま届けます。
①冷凍しないフレッシュ細胞
新鮮な、生きた細胞をそのまま投与するので生存率が高い
②脊髄腔内ダイレクト注射療法
数多くの幹細胞で直接傷ついた神経を再生
③1回あたり2億個投与
1億個×2回より高い効果が期待
④自己脂肪由来幹細胞
骨髄由来と比較して約2倍の神経修復効果(研究報告)
⑤自己血で培養
牛血清不使用でアレルギーリスクを最小化
⑥化学薬品を使わない培養
独自のシートでダメージを抑制し生き生きした細胞をつくる

生きたまま届ける「フレッシュ細胞」
幹細胞を冷凍せず、投与に合わせてその都度培養。
だから生存率が高く、効果が出やすいのです。

Our Strengths in Regenerative Medicine
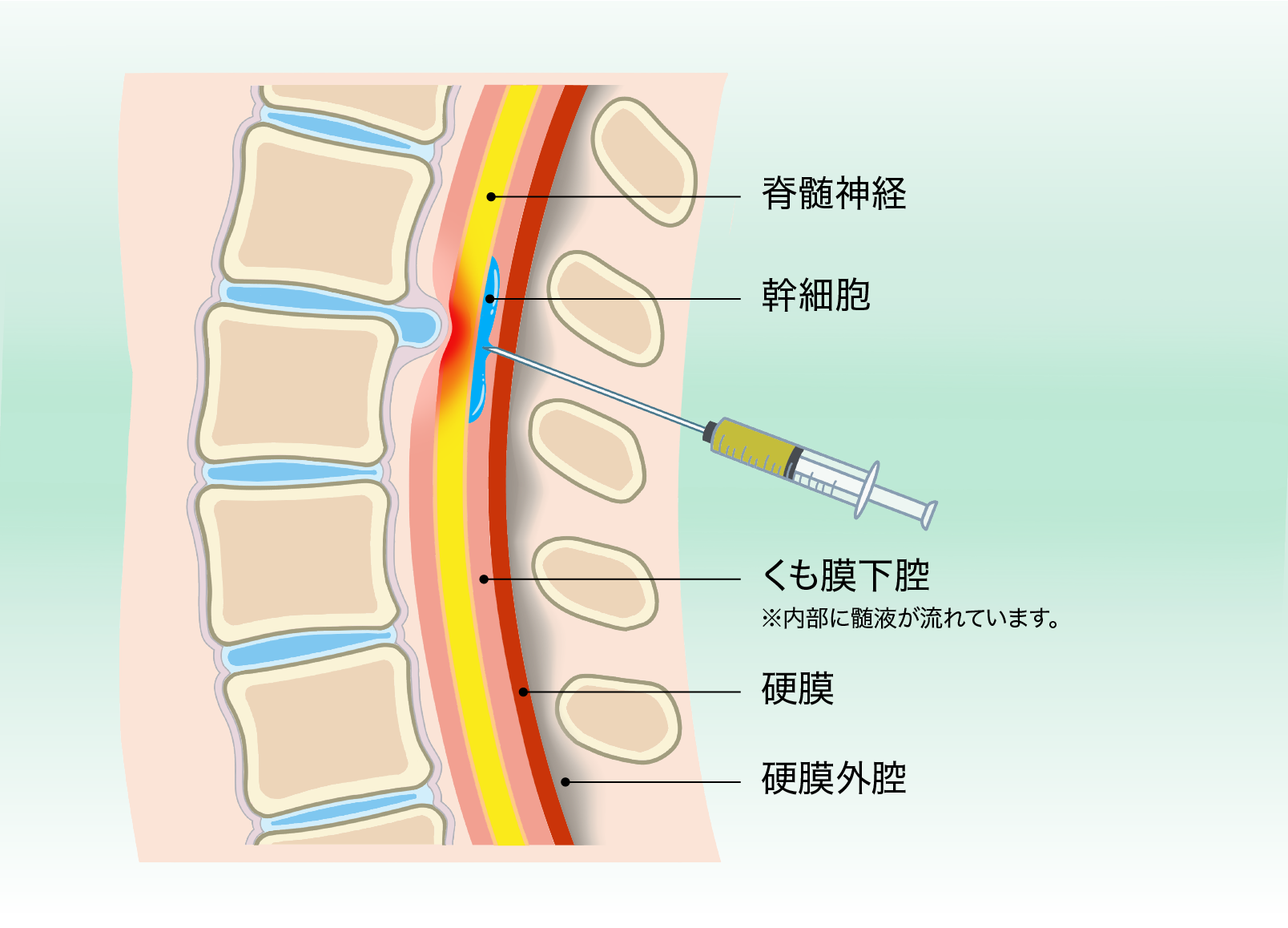
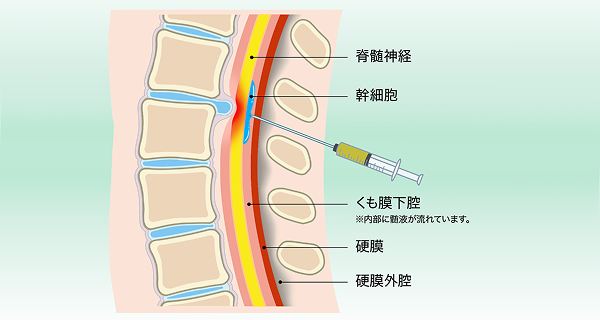
- 脊髄腔内ダイレクト注射療法 -
Stem cells are more effective at regenerating and repairing nerves when they're administered directly into the spinal cord cavity.
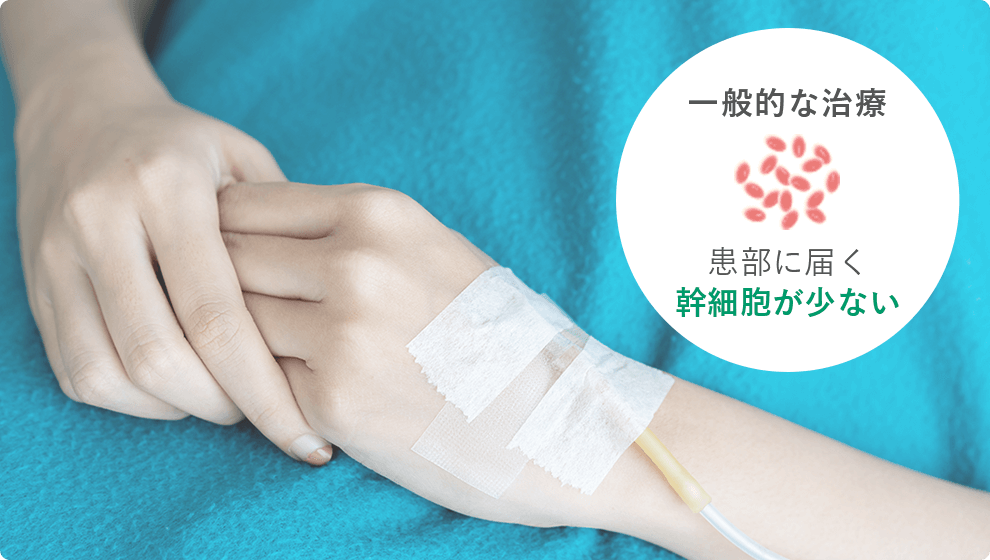
脊髄損傷の再生医療は点滴で幹細胞を投与し、血液循環を経て脊髄に到達させる方法が一般的です。
ただしこの方法では、血管内に注入された幹細胞が全身に分散するため、損傷した脊髄に届く際には幹細胞の数量が制限される傾向にあります。

Intraspinal Direct Injection Therapy
脊髄を包む膜の中(脊髄腔)に、
細い針で幹細胞を注射します。
After administration, stem cells flow into the spinal fluid.
髄液は脊髄の中を流れていますので、
脊髄の損傷部位まで幹細胞を届ける
ことができます。
治療も簡単な注射で数分だけの処置となり、
それほど痛みも伴いません。また、幹細胞の点滴と
併用することでさらなる効果が期待できます。
脊髄神経の再生や修復効果が高まるんだね!
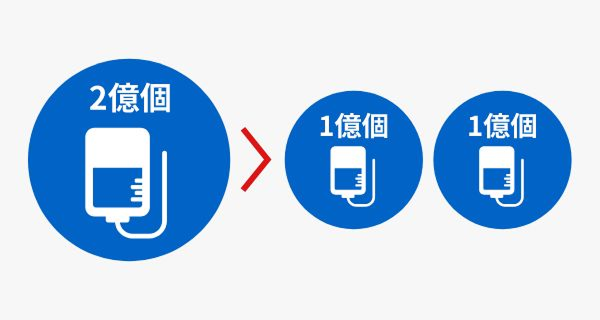
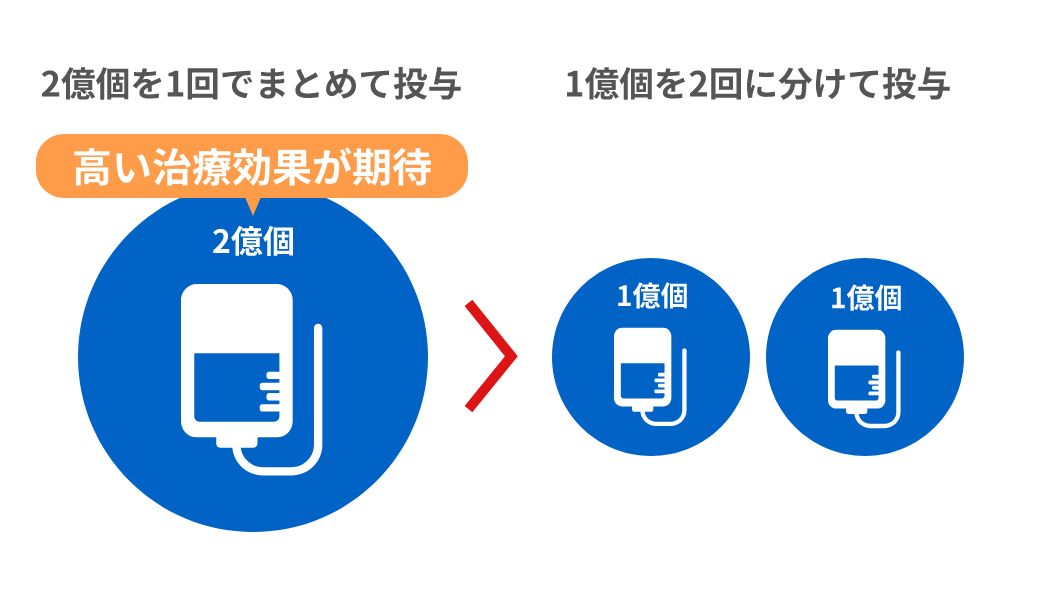
国内最高水準 2億個の幹細胞を
1回で点滴投与
合計投与量が同じ2億個であっても、1億個ずつ2回に分けて点滴投与するより、
2億個を1回でまとめて点滴投与するほうが高い治療効果が期待できます。
当院は、1億と2億の点滴治療を多数経験しているからこそ、効果の違いを実感しています。
1回の投与で2億個を投与することで、骨髄幹細胞を上回る神経再生が期待できます。
さらに、脂肪幹細胞は血管再生にも優れ、再発リスクの低減にもつながります。
投与方法による
効果範囲の違い
手術ではヘルニアの除去は可能ですが、傷ついた神経そのものを修復することはできません。リペアセルクリニックでは、脊髄腔内ダイレクト注射と点滴投与を併用することで、より広範囲の神経修復を目指します。
Intraspinal Direct Injection Therapy
- ●脊髄の傷ついた部位に幹細胞を直接投与
- ●脊髄付近の神経を修復
- ●直接投与するので効果が高い
点滴投与(静脈点滴)

- ●2億個の幹細胞が血液で全身に届く
- ●脊髄腔内ダイレクト注射療法で届かない場所や手足につながる神経を修復
- ●椎間板の悪化などを予防
- ●全身の臓器にも効果
脊髄腔内ダイレクト注射療法は局所に、点滴投与はダイレクト注射が
届かないところや全身に届くため、併用投与が効果的
脂肪由来の幹細胞
で神経・血管を修復
骨髄由来と比較して約2倍の治療効果が科学的に証明されています。
採取の負担も少なく、多くの細胞を確保できます。

なぜ脂肪由来なのか
- ✓骨髄と比較して採取が簡単で、患者様の負担が少ない
- ✓より多くの幹細胞を確保できる
- ✓神経と血管の再生・修復能力に優れている
- ✓高齢の方でも十分な細胞数を確保できる
国際研究20件が証明した
約2倍の治療効果
Scrollable
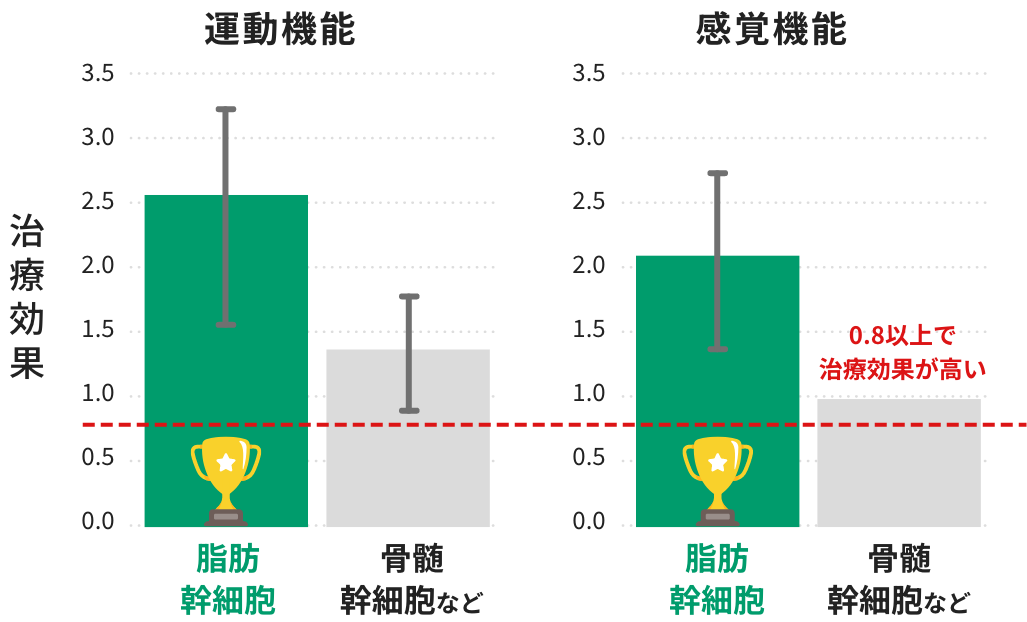
2020年の国際的な研究では、脂肪幹細胞は骨髄幹細胞と比較して血管新生・運動機能の向上・神経機能の再建において優れた成果を示すことが報告されています。
患者様ご自身の血液を使用し
代用血液を使わない安全な培養法
We do not use blood substitutes in cell culture.
代用血液
(牛血清、人工血清)

High safety and survival rates
当院では、ご自身の血液で培養するため、不純物や化学薬品などを含まず高い安全性と生存率が実現しています。
施設によっては、牛の血液や無血清培地という人工の血液を使用して培養するところもあります。


Generally, bovine blood and serum-free culture media are used for research purposes, but there are still concerns about allergies and mad cow disease in the clinical setting when actually administered to the human body.
In addition, although culturing stem cells from one's own blood requires advanced culturing techniques, stem cells cultured from one's own blood have strong vitality and can firmly repair damaged areas, enabling treatment with high regenerative potential.
幹細胞の抽出に先端技術
化学薬品・添加物を使わない独自の分離シート

当院では、長年研究を重ねて開発された独自の分離シートを使用することで、化学薬品や添加物を使わず、強い生命力を持った幹細胞を培養することが可能となりました。
ほとんどの医療機関では、従来の脂肪分解酵素(化学薬品)を使用した培養方法が主流で、これだと細胞が弱くなり生存率は低くなってしまいます。
さらに化学薬品となるため、アレルギーなどが懸念となります。
クリニックによって全然違うんだよ。
completely different tasting dishes depending on the cook and recipe.
培養ができるんだ。
これなら従来の脂肪分解酵素という化学薬品を使わなくて済むので、
アレルギーの心配がないんだ。
国内ではほとんど行われていないんだね。
さらに化学薬品を使わず、無添加なんてすごい!
これなら安心して身体に投与できるね。
さらなる生命力の強い幹細胞の培養を目指しているんだ!
当院では患者様の安全を第一に考え、幹細胞上清液(点滴療法、点鼻療法)、
サイトカインカクテル、エクソソームなどの製品は取り扱っておりません。

なぜなら、これらは他人から作られた場合が多く、他人の遺伝子物質が含まれる可能性があるため、十分な安全性の検証がなされていないからです。
また、自分自身のものであっても、これらの製剤は現行の再生医療等安全性確保法による規制対象外であるため、必要な安全基準を満たしているか確認できていない状況です。
第三者機関による
品質保証があるから
安心です
All stem cells confirmed to meet quality standards

幹細胞治療の
手順
At our clinic, stem cell therapy is performed according to the following procedure.
-

01
初診および問診(約2時間)
The physician will conduct a detailed investigation of the patient's condition and confirm whether stem cell therapy is suitable. After confirmation, the specific treatment process and details are explained, and if consent is obtained, a blood sample is drawn to test for infections and other diseases. After that, we will ask the patient to submit a consent form and start the treatment.
-

02
Fat collection (about 30 minutes)
患者様の下腹部に局所麻酔を行い、米粒3粒程度の脂肪組織を採取いたします。
-

03
Cell Culture Process
We have submitted a notification to the Ministry of Health, Labor and Welfare and professionally process adipose tissue collected at an accepted cell culture center into the specific cellular products required for treatment.
-

04
Stem cells are administered directly into the spinal cord cavity
- ・静脈点滴投与(約80分)
- ・局所投与(約5分〜)



治療にかかる標準的な
費用
明確な料金体系で、安心して治療を受けていただけます
Intraspinal Direct Injection Therapy
1回あたりの治療費
2,420,000円(税込)
セット価格や詳細はお問い合わせください
一度の治療で根本改善を目指す - 何年も通い続ける治療費・薬代・時間を考えると、
長い目で見ればご負担の軽減につながる可能性があります。
その他の費用
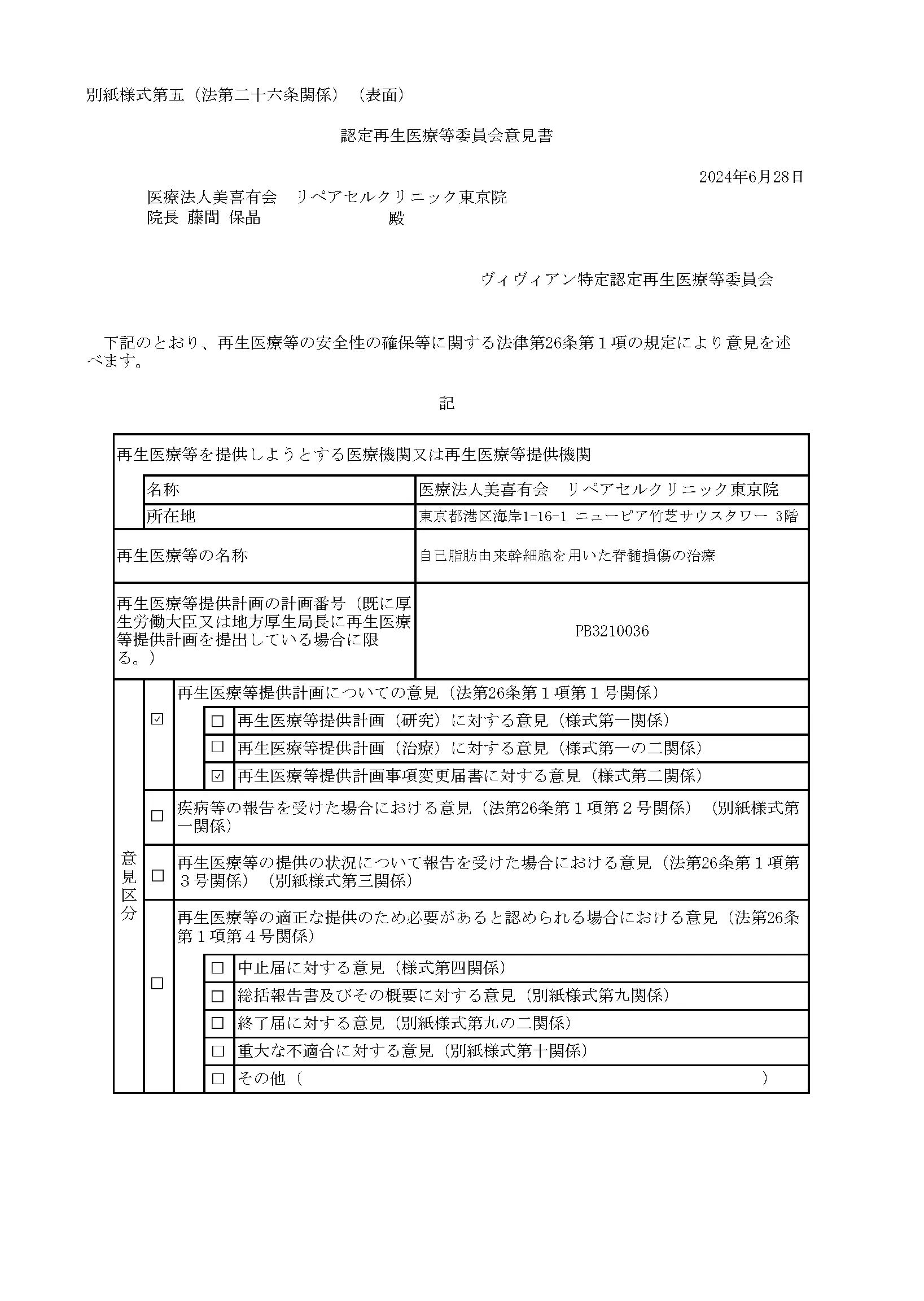
厚生労働省
届出済医療機関
Type 2 and Type 3 regenerative medicine provision plan Notified
届出書面「自己脂肪由来幹細胞を用いた脊髄損傷の治療」
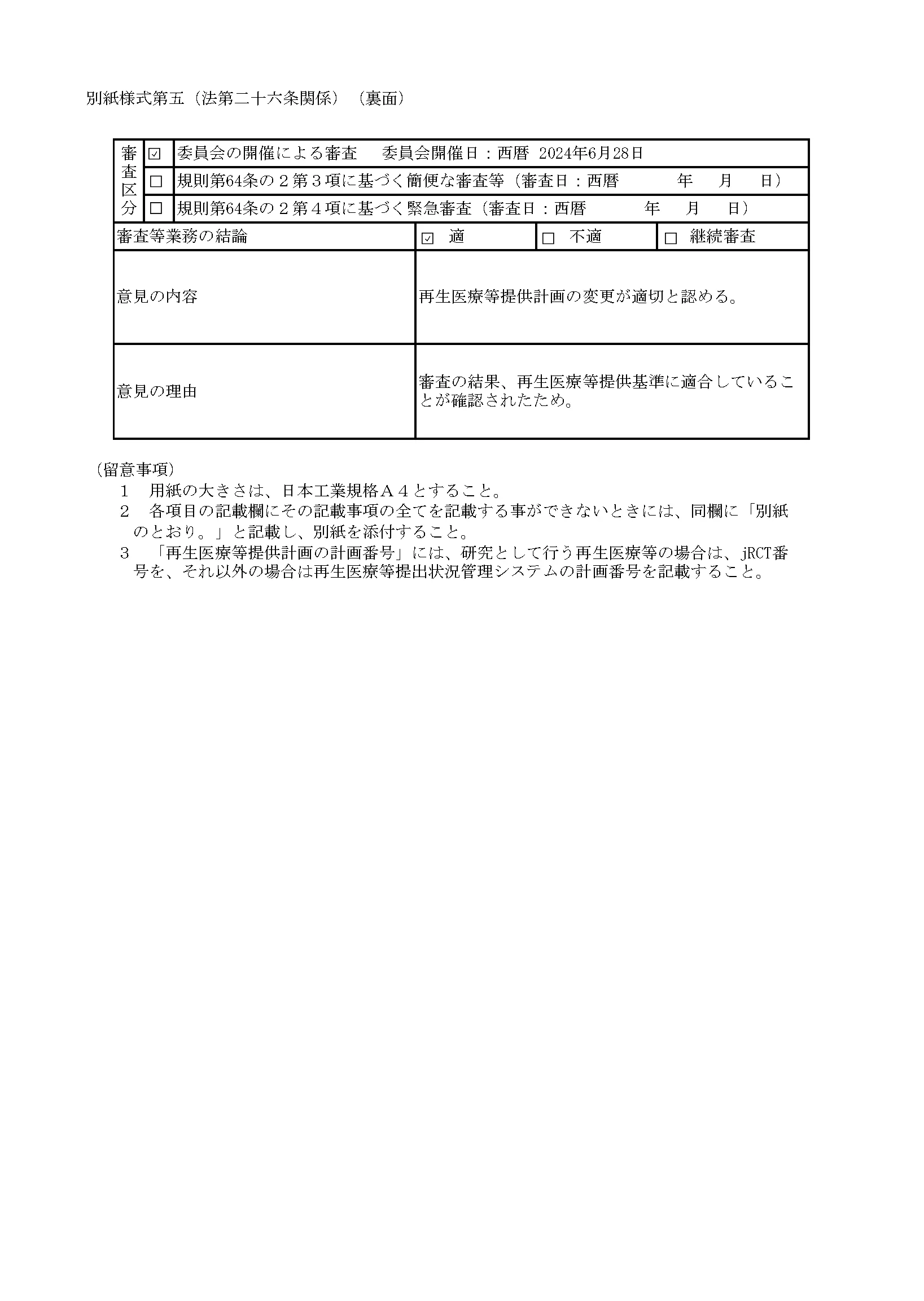
再生医療等安全性確保法施行規則に基づく届出
Treatment of spinal cord injury using autologous adipose-derived stem cells
リペアセルクリニックは、厚生労働省が認めた特定認定再生医療等委員会による厳格な審査を経て、治療計画を提出しています。
よくあるご質問
- この治療法は、本当に効果があるのでしょうか?
- はい、多くの方に症状の改善が見られます。痛み止めやブロック注射は一時的に症状を緩和しますが、
再生医療は「傷ついた神経そのもの」の回復を促します。
- 手術とどちらが良いのでしょうか?
- 手術は「圧迫の除去」、再生医療は「神経の回復」とアプローチが異なります。緊急の症状がなければ、
まず専門医にご相談ください。
- 手術をしたのですが、効果は期待できますか?
- はい、そのような方にこそ有効です。手術では取り除けなかった「神経の傷」に直接働きかけ、
さらなる改善を目指します。
- 症状が軽いのですが、治療を受ける意味はありますか?
- 症状が軽いうちからの治療は「予防的治療」として有効。将来的な手術のリスクを減らすことが期待できます。
- 副作用やリスクはありますか?
- ご自身の細胞を使用するため、拒絶反応やアレルギーのリスクは極めて低いです。注射部位の一時的な痛みや腫れが起きることはありますが、通常は数日で落ち着きます。詳しくはカウンセリング時に専門医がご説明します。
- 治療は何回受ければ良いですか?
- 多くの方が1〜2回の治療で改善を実感されています。症状の程度により異なりますので、
カウンセリング時に最適な回数をご提案します。
- 効果はどのくらいで実感できますか?
- 個人差はありますが、早い方で1〜2週間、多くの方は1〜3ヶ月程度で効果を実感されています。
神経の再生には時間がかかりますので、焦らず経過を見ていきます。
- 他院との違いは何ですか?
- 当院は「脊髄腔内ダイレクト注射療法」と「1回2億個投与」を組み合わせた独自の治療法を提供しています。
また、化学薬品や代用血液を使わない安全な培養にこだわっています。
- 遠方からでも通えますか?
- はい、日帰り治療が可能です。東京・大阪に拠点がございますので、全国からお越しいただいています。
宿泊が必要な場合は、提携ホテルのご紹介も可能です。
ご相談内容をもとに、あなたにあった治療法を見つけましょう
ご相談内容とMRI画像をもとに、専門医があなたの症状を詳しく診断します

専門医の診断でわかること
MRI画像から、あなたの症状が再生医療で改善できるか診断
必要な治療回数と、改善の見込みをお伝え
費用・通院頻度・回復期間をすべてご説明
無料電話相談 9:00〜18:00